Editorial: Radical prostatectomy at young age
Becker et al. [1] investigated a large sample of young patients (aged <50 years) who underwent radical prostatectomy during a 20-year period in a high-volume European centre. In this study [1], men aged <50 years had a significantly more favourable functional outcome (continence rates [0–1 pads] 97% vs 92%; International Index of Erectile Function [IIEF] score drop of 4 vs 8 points), compared with their older counterparts. Biochemical tumour control was higher in younger patients in univariate (5-year rates 81% vs 70%) but not in multivariate analysis.
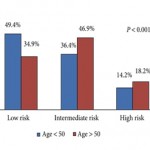
In studies in the pre-PSA era, young age at prostate cancer diagnosis was often associated with adverse tumour-related outcome [2]. Possibly, the disadvantage of younger patients was attributable to rapidly growing high-grade tumours causing symptoms at a young age in the absence of a dilution by favourable early detected low-grade cancers. In contemporary patients, the opposite is observed [1]. As the impact of age vanished after controlling for tumour-related prognostic factors reflecting the presence of more favourable disease criteria in younger men, it may be considered likely that PSA-based early detection enriched favourable parameters in the younger subgroup. Altogether, prostate cancer biology is probably not meaningfully associated with age. Outcome differences, even in randomised trials [3, 4], are rather caused by age-related differences in the approach to prostate cancer diagnostics and early detection than in actual biological differences.
The relative favourable functional outcome in younger patients [1] supports early curative treatment in this population. Currently available active surveillance studies have very limited follow-up and were performed mainly in elderly patients with significant comorbidity [5]. Currently, in Germany the further life expectancy in men aged 50 years is ≈30 years [6]. In a contemporary active surveillance study, narrowly half of patients received active treatment within 10 years [5]. Therefore, most men starting active surveillance at an age of 50 years will subsequently receive active treatment. This treatment will then be performed at a greater age where the chances for satisfactory functional recovery are less favourable.
The inferior tumour control rates in patients receiving robot-assisted surgery is another remarkable finding of this study (hazard ratio 1.4, 95% CI 0.99–1.9, P = 0.06 in the multivariate analysis). Although the significance level was narrowly failed, this observation cannot be ignored. It was accompanied by an increased continence recovery rate after robot-assisted surgery suggesting that it may probably not be attributed to the learning curve. Less radical removal of the prostate with more sparing of neurovascular structures and bladder neck might be a conceivable explanation of this phenomenon. In this study [1], the prognostic impact of robot-assisted approach was in a similar range as a positive surgical margin (hazard ratio 1.5, 95% CI 1.4–1.7).
Current clinical guidelines discourage prostate cancer screening in average-risk men aged <50 years [7]. It remains to be seen in which degree these recommendations will affect clinical practice and outcome parameters in this age group in the years ahead.
Manfred P. Wirth and Michael Froehner
Department of Urology, University Hospital ‘Carl Gustav Carus’, Dresden University of Technology, Dresden, Germany
References
- Becker A, Tennstedt P, Hansen J et al. Functional and oncological outcomes of patients younger than 50 years treated with radical prostatectomy for localized prostate cancer in a European population. BJU Int 2014; 114: 38–45
- Parker CC, Gospodarowicz M, Warde P. Does age influence the behaviour of localized prostate cancer? BJU Int 2001; 87: 629–637
- Bill-Axelson A, Holmberg L, Ruutu M et al. Radical prostatectomy versus watchful waiting in early prostate cancer. N Engl J Med 2011; 364: 1708–1717
- Froehner M, Wirth MP. Early prostate cancer – treat or watch? N Engl J Med 2011; 365: 568
- Selvadurai ED, Singhera M, Thomas K et al. Medium-term outcomes of active surveillance for localised prostate cancer. Eur Urol 2013; 64: 981–987
- Statistisches Bundesamt. Periodensterbetafeln für Deutschland 1871/1881 bis 2008/2010 [Period death tables for Germany 1871/1881 bis 2008/2010]. Wiesbaden 2012. Available at: https://www.destatis.de/DE/Publikationen/Thematisch/Bevoelkerung/Bevoelkerungsbewegung/PeriodensterbetafelnPDF_5126202.pdf?__blob=publicationFile [Website in German]. Accessed 12 July 2013.
- Qaseem A, Barry MJ, Denberg TD, Owens DK, Shekelle P; Clinical Guidelines Committee of the American College of Physicians. Screening for prostate cancer: a guidance statement from the Clinical Guidelines Committee of the American College of Physicians. Ann Intern Med 2013; 158: 761–769